You must be signed in to read the rest of this article.
Registration on CDEWorld is free. You may also login to CDEWorld with your DentalAegis.com account.
While the population is aging, so too are the treatment options for the edentulous patient. Today, osseointegrated implant-supported denture prostheses have eliminated many of the disadvantages associated with traditional dentures. The emotional impact of edentulism can be life altering, causing embarrassment, lack of self-esteem, an altered self-image, dissatisfaction with the facial appearance, and emotional insecurity culminating in social inhibition and difficulty establishing relationships.1
The physical effects of tooth loss include decreased oral facial support due to the loss of hard and soft tissue; the look of premature aging in the facial region caused by bone resorption; a decrease in lip support and facial height; impaired phonetics and oral function; and pain.2 These physical issues contribute to the discomfort and ultimate instability of conventional removable denture prostheses by requiring the denture wearer to use the lip, tongue, and cheek muscles to hold traditional dentures in place.3,4
Implant-retained dentures resolve many of these issues. For instance, patients experience a secure and stable fit, better comfort, improved biocompatibility, increased support, and decreased bone loss when two to four implants are placed to support a full-arch prosthesis.3,5 In addition, improved material sciences have provided newly developed denture-based technology and denture tooth materials that are stronger, more esthetic, and last longer than even natural teeth.
Case Presentation
A 63-year-old woman presented with upper and lower partial dentures (Figure 1). She had become frustrated with the lack of stability of the partials and the failing abutment restorations. She was also concerned about her appearance. The patient’s present health condition was documented, which included arthritis, chronic lower back pain, chronic narcotic use, and hepatitis. The patient was presently on a regimen of Celebrex, Fiorcet, and oxycodone. It was also noted that the patient had an allergy to codeine.
After a clinical examination was performed including diagnostic digital radiographs (Figure 2), diagnostic study models, photographs, and a CBCT scan, treatment options were discussed and the patient’s future expectations were addressed and documented. She had received a previous treatment plan and had been told she needed a sinus lift and a bone augmentation but decided against them. Her desire was to have a fixed solution so she would not have to remove her denture teeth.
Treatment Planning
Three-dimensional implant-planning software is a safe and accurate tool to achieve implant placement. In this case the dental team used SimPlant® software to create a virtual treatment plan that included extracting all the teeth and placing four implants on the upper and lower arches using the All-on-4 technique. Because this technique can accommodate a wide range of prosthetics and abutments, and it also allows immediate-supported restorations by directly attaching a provisional prosthesis onto the implants after surgery.6-10 This was agreed upon treatment for this case. Accurate bite registration and mounted casts were also performed for further treatment planning.
Conventional impressions of the upper and lower arches were performed for the laboratory technician to begin construction of the immediate dentures using the patient’s current dentition as a guide for tooth position. These dentures would then be modified into screw-retained provisionals at the time of surgery (Figure 3 and Figure 4). Using the immediate denture as a guide, a clear replica was fabricated for use as the surgical template.
Implant Placement
Vertical dimension of occlusion was recorded before anesthetizing the patient with IV sedation containing 75 mg of Demerol, 12.5 mg of Versed, 2% Xylocaine 1:100,000 epinephrine, and 0.5% Marcaine 1:200,000 epinephrine. Extraction of teeth Nos. 3, 5, 6, and 7 from the maxillary was performed first, followed by maxillary alveoplasty. Next, a hole was created from the anterior wall of the floor of the left and right sinus. Implant placement was performed with the aid of a surgical template (All-on-4). A 2-mm drill site was created midline and an implant stent was placed. Next, a posterior implant, at no more than a 45° angulation, was placed 4 mm in front of the sinus. The head of the implant in the second bicuspid area was emerged (4.3 mm x 15 mm). The drill sites were left underprepared, especially in the maxilla. A 30° multiunit angled abutment was placed. Two straight anterior implants were placed into the nasal floor (4.3 mm x 13 mm) and the maxillary anterior implant was placed at a 17° angle. The angled implants would accommodate for the lack of healthy bone structure by increasing bone-to-implant contact.
Mandibular teeth Nos. 22 through 27 were extracted and a radical mandibular alveoplasty was performed leaving approximately one quarter of the extraction sockets remaining. Having located the right and left mental foramen nerve, a 2-mm drill site was created midline and the implant stent was placed. Two 30° angled implants were placed in the mandibular second bicuspid area—right 4.3 mm x 18 mm and left 4.3 mm x 18 mm at no more than a 45° angulation. Next, straight implants were placed, right 4.3 mm x 13 mm and left 3.5 mm x 13 mm. Finally, the anterior implants were placed at a 17° angulation. Multi-unit abutment healing caps were placed onto the abutments.
Upper and lower immediate dentures had been prepared prior to surgery by the dentist and laboratory technician. The maxillary was tried-in using the palate as the constant to verify incisal edge position and fit. A putty bite was used to stabilize and verify occlusion with any remaining mandibular teeth that had yet to be extracted. After suturing around the healing caps, the sutures were covered with Vaseline®, and a rubber dam was adapted around the healing caps to protect the sutures during the acrylic curing.
A fast-setting, hard-denture chairside reline material was applied over the white caps to locate the position of the eventual screw access holes. This reline also provides hard-processed tissue stops between the implant/abutment sites. Based on the location of the healing caps, the laboratory technician would drill holes through the tissue side to the occlusal side of the teeth.
Titanium provisional sleeves were placed on the multi-unit abutments and picked up with the fast-setting chairside reline acrylic that was injected around each sleeve using monoject syringes while holding the prosthesis in place. The prosthesis was held in position until the acrylic was fully set. The screws were then removed from the sleeves, and the entire overdenture was removed with the sleeves embedded into the acrylic. Any voids around the tissue side of the temporary sleeve would be filled in by the laboratory technician. The facial flanges and the palate were removed from the overdenture. The immediate provisional must not have any ridge laps or un-cleansable areas during healing.
While the maxillary immediate was being converted into the provisional, the oral surgeon performed extractions of the mandibular teeth and implant/abutment insertion. The same conversion steps were used on the mandibular denture using the already inserted and stabilized maxillary provisional for occlusion and position.
The patient was allowed to heal, and postoperative follow-up treatments were performed until osseointegration was complete (Figure 5 and Figure 6). Three months later, the provisionals were removed and abutment-level impressions were taken for the definitive restoration. Pickup impressions of the provisional prosthesis served as verification jigs and were mounted. While the patient waited for the return of their temporary restorations, tooth selection and shape were discussed, agreeing upon a polymethyl methacrylate acrylic material (PMMA), known for providing long-lasting restorations. While earlier generations of denture teeth were likely to fracture, Mondial® Denture Teeth (Kulzer, www.heraeus-dental-us.com) were chosen in this particular case due to their voidless, high-density center specifically designed to accommodate the opening for the insertion of the screw without weakening, for screw-retained prostheses. Alternatives include: Phonares® (Ivoclar Vivadent, www.ivoclarvivadent.com), Portrait IPN (Dentsply Sirona, www.dentsplysirona.com), and others.
Denture Fabrication
A radiograph was taken to verify that the provisional with temporary sleeves was adapted perfectly to the shoulder of the multi-unit abutment as this prosthesis was used as the verification jig (Figure 7). The composite implant plug was removed to gain access to the multi-unit abutment screws that were then removed. Twenty-millimeter guide pins were inserted through the provisional. The patient could not close her mouth at this point.
Using a stock tray, holes were drilled so that the 20-mm guide pins could pass through the tray, and an open-tray impression of the prosthesis could be taken using PVS material such as Flexitime® (Kulzer), Aquasil Ultra (DENTSPLY Caulk, www.caulk.com), or Hongium® (DMG America, www.dmg-america.com). The purpose of this impression was to record any discrepancies between the healed tissue and the provisional during the 3-month integration period. Once the impression was set, the guide pins were removed. The impression was then removed with the prosthesis still embedded. A plastic healing cap was placed on the multi-unit abutment while the provisional was out of the mouth for approximately 1 hour as the case was poured and mounted.
To complete the pour-up of the impression with the provisional still embedded, multi-unit analogs were screwed on and the 20-mm guide pins were used. A removable soft-tissue material, required during the scanning process by the bar manufacturer, was poured around the analogs and then the balance of the impression was poured up with regular die stone. The impression was unscrewed from the model and separated. The prosthesis was removed from the impression and placed back on the master cast with laboratory multi-unit abutment screws. The case was then mounted onto the articulator.
Three appointments for the restorative dentist were eliminated by using the provisional as a verification jig and by using the prosthesis mounted on the master cast for vertical dimension and tooth try-in. The articulator was set, and the provisional was removed and returned to the dentist for insertion.
Laboratory Fabrication Techniques
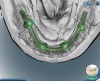
The laboratory technician made a small triad base-plate using at least two titanium provisional sleeves into the base plate. This allowed the restorative dentist to stabilize any required intermediate tooth try-ins. The teeth were set up, and a wax-up of the facial contours was produced. The facial and lingual contours of the wax-up were created as an exact replica of the finished product. The teeth were removed from the wax-up leaving a negative of the denture teeth in the wax around the arch. The master cast and baseplate without the teeth were forwarded to the bar manufacturer for scanning. Due to the fact that this particular technique and the implants can accommodate a wide range of prosthetics and abutments, high-strength zirconia or titanium substructures can be fabricated using CAD/CAM technology (Figure 8 and Figure 9).10,11 Therefore, the bar was designed on screen considering support for each tooth, and then it was milled and returned to the laboratory.
At this point, the denture teeth were reset into the baseplate wax-up. A laboratory stone facial matrix was taken of the set-up, and the teeth were boiled off the baseplate and replaced in the stone matrix. The milled bar was then screwed on the master cast. The stone matrix with the denture teeth was verified on the front of the master cast to ensure that no contact between the titanium bar and the denture teeth was made, and the prosthesis was designed with proper support. Modifications were made to the teeth and titanium bar as needed. The bar was then removed from the model and sandblasted with aluminum oxide.
A metal primer and a pink, light-cured opaque were applied to the framework to mask the gray metal bar. The matrix with teeth was returned to the master cast, and the teeth were attached to the framework using baseplate wax applied with a hot eye dropper. The matrix and framework were removed from the model and any voids were created to replicate the finished contours. At this point, the case was returned to the restorative dentist to be tried in while the teeth were set in wax on the titanium framework. After being approved by both the dentist and patient, the case was returned to the laboratory and was invested and processed using conventional denture procedures. Care should be taken not to allow acrylic to enter the screw access holes or abutment receptacles on the tissue side of the prosthesis. After screw access holes were drilled and sized for a passive insertion of the abutment screw, the prosthesis was returned to the restorative dentist for final delivery.
Delivery
Upon delivery, the prosthesis was screwed into the implants and torqued to 15 Ncm. The screw access hole was filled with a plugging material to within 1 mm of the top of the sleeve. Composite material was then used to bring the screw access hole level with the surface acrylic. The procedure was repeated for the lower denture (Figure 10 and Figure 11).
Conclusion
With today’s implant-supported denture treatment options, both the physical and emotional affects of edentulism can be eliminated. Advanced materials and procedures allow dentists to offer their patients restorations with optical and functional qualities that mimic those of natural dentition while providing improved fit and biocompatibility. The use of CAD/CAM technologies decreases the time involved and increases the ease of the restorative procedure while attaining exceptional accuracy, and enhanced material properties increase durability and longevity providing edentulous patients with premium quality dentition. In addition, in extensive procedures like this one, patients’ chairtime can be reduced with resourceful techniques such as using the prosthesis mounted on the master cast for vertical dimension and tooth try-in, and using the provisional as a verification jig, benefiting both the patient and clinician by minimizing patient visits.
References
1. Fiske J, Davis DM, Frances C, Gelbier S. The emotional effects of tooth loss in edentulous people . Br Dent J. 1998;184(2):90-93.
2. Vogel RC. Implant overdentures: a new standard of care for edentulous patients current concepts and techniques . Compend Contin Educ Dent. 2008;29(5):270-276.
3. Henry K. Q&A on the future of implants . Dental Equipment and Materials. 2006; September/October.
4. Rossein KD. Alternative treatment plans: Implant-supported mandibular dentures . Inside Dentistry. 2006;2(6):42-43.
5. DiMatteo A. Dentures and implants: Bringing them together for a winning combination . Inside Dentistry. 2009;5(1)97-104.
6. Agliardi E, Panigatti S, Clericò M, et al. Immediate rehabilitation of the edentulous jaws with full fixed prostheses supported by four implants: interim results of a single cohort prospective study . Clin Oral Implants Res. 2010;12(5):459-465.
7. Maló P, Nobre Mde A, Lopes I. A new approach to rehabilitate the severely atrophic maxilla using extramaxillary anchored implants in immediate function: a pilot study . J Prosthet Dent. 2008;100(5):354-366.
8. Maló P, de Araújo Nobre M, Lopes A, et al. A longitudinal study of the survival of All-on-4 implants in the mandible with up to 10 years of follow-up . J Am Dent Assoc. 2011;142(3):310-320.
9. Cehreli S, Ozçirpici AA, Yilmaz A. Tilted orthodontic micro implants: a photoelastic stress analysis . Eur J Orthod. 2011 Jul 11. [Epub ahead of print].
10. Maló P, Rangert B, Nobre M. All-on-4 immediate-function concept with branemark system implants for completely edentulous maxillae: a 1-year retrospective clinical study . Clin Implant Dent Relat Res. 2005;7(Suppl 1):S88-S94.
11. Irinakis T, Wiebe C. Clinical evaluation of the nobelactive implant system: a case series of 107 consecutively placed implants and a review of the implant features . J Oral Implantol. 2009;35(6):283-288.
Author the Authors
David A. Little, dds
Professionals in Dentistry
San Antonio, Texas
Steven B. Buckley, dds, md
Alamo Maxillofacial Surgical Associates
San Antonio, Texas
Randy Saunders, cdt
Natural Arts Dental Lab
San Antonio, Texas